Need to Go to Plastic Surgeon to Have My Chest Incision Opened Again N Cleaned Out N Closed Up
Medical students and foundation doctors are notorious for not knowing how to conduct in the operating theatre. This is almost invariably considering nobody always bothers to tell yous how information technology all works, what to await and what to practise with yourself; instead, they merely expect yous to somehow instinctively intuit the rules governing what is a very complex working environment. This means most students and junior doctors get very little out of their often limited theatre exposure, and as a effect are deeply bromidic past the whole surgical thing, which I find really sad.
To rescue y'all from potential clumsiness and embarrassment, I've put together a listing of simple things I wish I had known when I was a student. Most of these are things that I got shouted at for not doing/non knowing and therefore learned near the hard way, my aim is to save y'all from having to get through this. Information technology's very piece of cake to experience like little more than an inconvenience in theatre, but the informative tips beneath volition hopefully assist y'all learn lots, and you lot might even savor yourself!
Y'all might besides be interested in our surgical flashcard collection which contains over 500 flashcards that cover key surgical topics.
Before the operation
Arrive on fourth dimension; aiming to be almost 15 minutes early is best. This is a simple betoken, but arriving late will brand a bad first impression and the team may disappear off to the mysterious and inaccessible land of "theatre" without you lot. Information technology is generally a good thought to be well-rested and not hungover.
Earlier going to theatre, the registrar or consultant will go and see the patients to take them through the consent form and marking them for the operation if necessary. It is best to get with them if you lot tin. Information technology volition make a proficient impression on the team, and it likewise ways that you will get to see the patient while they're actually awake and see their "patient journey" through. Pay attention to the consent process, as y'all volition learn the answers to some common intra-operative interrogation questions, including what the process involves and any common or serious complications.
After all the patients accept been seen and consented, it'southward time to go and go changed. If y'all are going to exist separated from your team at the changing room door, brand sure y'all know which theatre you need to become to when y'all become to the other side! If you can't get into the irresolute rooms, get to the master desk, explain who you are and where you're going, and a nice person should allow y'all in.

Theatre attire
Hither are a few fundamental points about theatre attire…
Scrub colours
On entering the changing room y'all will probably be confronted by a veritable rainbow of different-coloured scrubs. For example, my hospital hasgreens for full general wear in theatre, dark dejection for theatre sisters, light dejection for general clothing outside of theatre, orange for healthcare assistants, pinkish for obstetrics and gynaecology, and gray for ITU doctors. The colours used will vary betwixt different hospitals (I've rotated around a lot over the past few years and have as well worked in places that but use royal blue, raspberry or turquoise scrubs), and then check the local policy with someone if you're not certain which ones y'all're meant to wear.
Scrub sizes
There should be a coloured band around the neckband of the scrub tops and the waistband of the scrub trousers to indicate what size they are. In my infirmary, yellowish is small, brown is medium, blueish is large, white is actress-large, pink is XXL and reddish is XXXL. Again, this may vary depending on which scrub visitor your hospital uses. There is often a helpful mitt-made size guide that ane of the nurses has stuck to the wall somewhere – check the toilets if you tin't find it!
Shoes
There should exist a selection of rather unfashionable clog-similar rubber theatre shoes available for y'all to put on. Don't take any with people'due south names or initials written on, every bit you volition be in trouble if they take to come looking for them! If there aren't whatever spare shoes, don't be scared to ask somebody at the front desk to see if they can find some for you. It is very important that y'all don't article of clothing your own shoes into theatre, for several reasons. Firstly, tramping mucky trainers into theatre is plainly not good for infection control. Secondly, theatre shoes are specifically designed to stop you from slipping on wet floors and from getting zapped by the diathermy. Finally, and perhaps most importantly, wearing theatre clogs protects your own shoes from getting covered in horrible theatre mess. As a quaternary-year medical student, I once had to squodge 2 miles domicile in trainers drenched with stinky amniotic fluid after assisting with an elective Caesarean section list. Trust me, one time you lot've had that experience, you lot'll never desire to do it again!
There may besides be wellies in the changing rooms. Don't habiliment these – they're for the urologists. I'll leave it to y'all to figure out why.
Hats
You lot will need to clothing a hat to cover your hair. Confusingly, these also come up in an array of colours for different squad members, which may or may not friction match their corresponding scrub colours in any manner. Medical staff volition usually wear blue hats, but sometimes students are asked to habiliment a different colour instead – again, at that place should exist a handy guide stuck to the wall somewhere! There are ii types: stretchy rubberband-backed ones, and ones that necktie in a knot at the back of your head. Make sure all devious bits of hair are tucked underneath your hat, otherwise, you lot run the risk of the theatre sister being less than impressed with you. If you have a bristles, in that location should be special hats for you with a funny extra bit to cover the beard expanse.
Jewellery
The general rules for jewellery are the aforementioned in theatre as they are on the wards. You lot must be "bare below the elbows" with the exception of a plain wedding ring if y'all're married – plainly, the holy and sacred nature of wedding vows prevents these rings from spreading any infections. If you're wearing earrings, I would either take them off or constrict them under your hat, as they have been known to occasionally fall off into patients. If you have any other visible piercings, be sensible about what you wear to work.Necklaces are usually fine as long as they're not massive or offensively blingy – I've worn ane every 24-hour interval for over a yr at present and it's never been a trouble.
Magic gowns
For infection control purposes, you are not supposed to exit the theatre surface area wearing your greens. If you need to pop out for any reason, at that place is usually a stash of green gowns near the doors which will human activity to cover your scrubs and magically forestall you from acquiring any transmissible leaner during your time away from theatre. These are also extremely comfy to wear and permit y'all to swoop dramatically around the hospital like some kind of cape-wearing surgical superhero. Y'all'll come across most people wear them similar a dressing gown with the opening at the forepart, merely you lot're actually supposed to wear them like a theatre gown with the opening at the back and the strings tied deeply. Some hospitals may require you to actually get changed to leave theatre, and so bank check the local policy if you're not certain.
Information technology tin can be hard to detect somewhere to put your thingswhen you're not a regular fellow member of staff – I'm a surgical trainee and I nevertheless can't get a locker! Your clothes and shoes volition normally be fine left in the changing rooms – I usually put them folded in a little pile under a bench or on a windowsill; avoid the tops of the lockers as things tend to get very dusty up there. However, you will desire somewhere safe to go along your bag and other valuables. Nigh theatres will have lockers available for visitors, but yous will often exist on a tight schedule and information technology tin take a while to detect the person with the keys! Instead, I usually bring my bag into the theatre and inquire the nurse in accuse if information technology'due south OK to get out it in a corner out of the way. This has never been a problem as long as I accept asked get-go.
Each operating theatre will consist of several different areas; usually, a scrub room with sinks where the nurses and surgeons get scrubbed upward, an anaesthetic room where clever people put patients to slumber, a littlestoreroom with basic equipment like sutures and staplers, and the theatre itself. This means yous will be confronted with several potential entrances when you arrive. Just recall that you should never open any doors that go direct into the theatre during an operation, every bit this could let in airborne contaminants that might land in the patient. For simplicity, I always use the scrub room door whether or not an operation is taking place.
When you get inside your theatre, innovate yourself to everyone, explaining who you are and your form or role. This will encourage people to look after y'all and might get y'all cups of tea and/or block if bachelor (anaesthetists tend to be awesome at baking). Make sure your name badge is clearly visible. Whatever yous exercise, don't cower silently in the corner looking like a lemon. The nurses and ODPs might seem stressed and scary, but in bodily fact, they are lovely difficult-working people who will welcome anyone who seems dandy and friendly.
This may seem obvious, but don't utilise your telephonein the operating theatre. Put it on silent and leave it in your bag – there will always exist chances to check it in the coffee room between cases.
This may seem even more than obvious, only for God'due south sake don't fifty-fifty call up of taking photographs !
Theatre lists should start with a "team brief" where everyone (e.g. surgeons, anaesthetists, nurses, ODPs, surgical practitioners, medical students, company reps) introduces themselves and their role. The team, led by the surgeon and anaesthetist, then discuss the cases for the twenty-four hours, including the order of the listing, the positioning, drugs and equipment that are required, and whatsoever specific bug and risks for each patient. The team brief is often affectionately referred to as "the hug" or "the huddle", then if anyone walks in and asks "shall nosotros hug?" or "have nosotros huddled yet?" this is what they hateful!
Later the team brief, the outset patient will be "sent for" from the ward and most of the team will launch into action. The floor nurses and ODPs go the necessary equipment set up, and the designated scrub nurse for the operation gets scrubbed to open and prepare the instrument trays. Meanwhile, the anaesthetists and their assistants scissure on with putting the patient to sleep. If y'all're anaesthetically inclined, yous could always ask to go in and watch this. The surgeons may loiter in theatre or go for a java depending on how long this is likely to accept, which is dictated by the complexity of both the patient and the procedure.
Always have a bite to consume and something to drinkable before the kickoff case starts, and Ever bring lunch for an all-day list. The surgeons go for a coffee while they're waiting for a reason! You will exist surprised how tiring it is standing upwards and concentrating for long periods, and operations often accept longer than expected for various reasons. Hunger and hypoglycaemia mean shaky hands, slowed reflexes and generally poor outcomes of intra-operative grilling sessions from consultants. The prolonged standing, heavy scrub gowns, gloves, masks and hot vivid lighting can mean yous also get overheated and dehydrated very chop-chop. Fainting is a genuine risk, and often happens to the final person y'all would look (east.one thousand. the vi-foot-something rugby players) so brand sure you await later yourself. If yous end up going the whole list without peeing, you lot aren't drinking enough!
Speaking of peeing, it's e'er sensible to go to the loo before starting a long operation.
Preparing for the operation
Preparing the patient
One time the patient is comatose and the anaesthetist has established all the necessary intra-operative monitoring, they are brought into the theatre. If a catheter is required, the nurses or surgeon volition unremarkably do this – if you've had some experience of catheterisation you could offering to insert it for them under supervision.
It takes several people to move the patient from their bed to the operating table with the anaesthetist giving instructions and controlling the airway, IV access and other attached monitoring. This is something you tin can assist with which will brand a very skilful impression. The procedure unremarkably requires the use of a PatSlide, which is basically a plastic board used to slide the patient beyond from the bed to the table.
Here is a charmingly 80s video from Ross Mannion on YouTube illustrating how this is done (nowadays nosotros usually need two people on either side equally our patients are getting heavier).
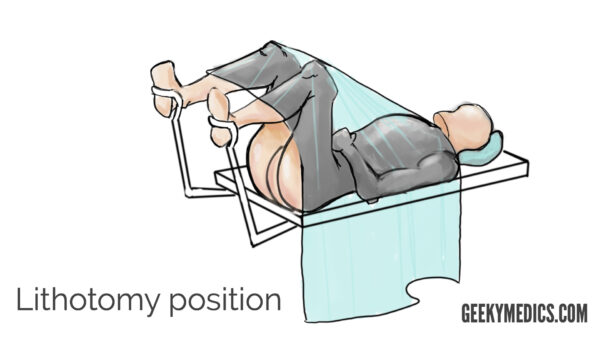
Once the patient has successfully reached the operating tabular array, the patient is positioned for surgery. In that location are many different positions which provide access to different parts of the body, and the operating table tin can move and have parts added or removed to accommodate these. The patient needs to be deeply strapped to the tabular array so they don't fall off if it gets tilted and should take adequate padding provided to minimise the hazard of pressure sores or nerve injuries. The surgeons unremarkably assistance with this but they might go to scrub while the rest of the squad do information technology. It is skilful practise to inquire the anaesthetist's permission earlier positioning the patient and to maintain the patient'due south dignity as much as possible by minimising exposure.
Scrubbing, gloving and gowning
Every bit a medical student or supernumerary fellow member of the team, it is adept practice to wait to exist invited to scrub in. If you lot appear to have been forgotten about, you tin always enquire permission to scrub in and assist – the worst that tin happen is that they will say no, but almost surgeons volition appreciate the initiative and the ones who don't are less likely to be keen on teaching anyway.
Bank check out our scrubbing, gloving and gowning guide for more details.
If you can't scrub in due to in that location being too many people/an unenthusiastic surgeon, you can either stand up on a step to sentinel or go hang out with the anaesthetist instead. Anaesthetists are a friendly brood of caffeinated super-nerds who tin teach you lot nigh all sorts of clever things that surgeons don't have a clue about, such equally breathing tubes, millimoles, sodium, ECGs and Poiseuille'south constabulary.
Here is a totally awesome video past Celine Lakra on YouTube, wherein a lady with perchance the nicest vocalization ever shows y'all how to scrub, glove and gown properly.
Some key points that I would add to this are:
- There are three main dissimilar coloured scrub solutions available: povidone-iodine (Betadine), chlorhexidine (Hibiscrub) and triclosan (SkinSan). I always apply Iodine, every bit I find it the to the lowest degree irritant and information technology makes information technology really easy to see that you've covered every last scrap of skin whilst you're scrubbing. Whichever one yous choice, stick to it, as mixing the solutions can lead to a actually nasty dermatitis.
- Your first scrub of the 24-hour interval must ever be a full 5-infinitesimal scrub. Afterwards this, any subsequent ones can be an abbreviated three-minute scrub, provided you have non done anything in between procedures that could grossly contaminate your easily (e.g. going to the toilet or eating lunch).
- Don't ever blitz scrubbing in or cutting corners – theatre staff pay close attending to this, and also as potentially earning you a telling off, it volition put the patient at take chances of a potentially catastrophic surgical site infection.
- If you lot accidentally bear on anything non-sterile at whatever bespeak, yous have to start all over again!
- Always wear a visor mask to protect your optics – you volition exist absolutely kicking yourself if you end up getting an heart-splash! I speak from experience: when scrubbing for an emergency C-department once I couldn't find where the visor masks lived and I was besides scared to ask, so I went without and got a faceful of blood.
- Most hospitals now promote double-gloving for surgical procedures, as it provides increased protection against needlestick injuries and claret-borne virus transmission. Yous can either put on two pairs of normal gloves (I would recommend 1 of your size and then 1 of the adjacent size up) or there may be "indicator" gloves available with a green or blue nether glove and a normal white top glove, so you can easily spot if your glove has been torn or pierced. A lot of consultants opt not to double-glove purely because it makes information technology much more than hard to experience frail structures inside the body, merely as an assistant, it shouldn't impair your function to any meaning extent, and so I would definitely practice it.
WHO Surgical Condom Checklist
The WHO Surgical Safety Checklist was introduced in 2008 and has since revolutionised patient prophylactic and the whole civilisation of surgical exercise across the world. It was designed to make sure surgeons operate on the correct bit of the correct patient with valid consent, equally well every bit to reduce common preventable causes of operative morbidity and mortality such every bit badly administered anaesthetics, allergic reactions, bleeding and infection. To summarise, the checklist is completed at iii primal points:
- "SIGN IN"– before the patient is put to sleep in the anaesthetic room, the anaesthetist confirms the patient's identity and the procedure they have been consented +/- marked for, as well as checking for whatsoever allergies or airway bug and making sure all their equipment is working.
- "TIME OUT" (also known as the "knife check") – before the performance starts, the whole team stops what they are doing to confirm the patient's identity and check the consent class, as well every bit discussing a range of other variables such every bit haemorrhage take a chance, antibiotic requirements and VTE prophylaxis.
- "SIGN OUT" – before the patient leaves the theatre, the nursing staff confirm that all instrument counts are correct, all specimens are correctly labelled and whatever issues around the patient's mail service-operative recovery accept been addressed.
The team cursory at the start of the day is also part of the process. If you want to acquire more virtually it and why information technology's so important, read "The Checklist Manifesto" by Atul Gawande.
Prepping, draping and the sterile field
Subsequently the knife bank check, the patient is prepped and draped. This involves cleaning the skin with an antiseptic solution such as iodine or chlorhexidine, which is applied and left on to dry. Hairy patients ofttimes need to be shaved before the peel is prepped. If monopolar diathermy will be used, the diathermy pad is placed on an area of salubrious skin. A warming device like a Bair Hugger™ might as well be placed over the patient. Next,adhesive surgical drapes are applied to outline the surgical field (e.g. the abdomen or leg) and cover up the rest of the patient and the operating table.
Whilst waiting for the patient to be prepped and draped, stand up with your easily clasped in front of you lot at chest or waist meridian to stop yourself from touching anything muddied. You lot will discover that most surgeons will actually stand up with their artillery folded, which seems to exist a generally accepted alternative but carries a potential chance of contaminating yourself on the "muddy" back of your gown.
Always ask the consultant where they would like you to stand, they might want their assistant opposite them or adjacent to them depending on the procedure.
Once the patient is draped, you can approach the tabular array. Information technology is important to be aware of the sterile field and what you are immune to touch. Things you lot tin can touch include the front end of your gown to a higher place your waist, the prepped surgical field, the draped area and whatever instruments the scrub nurses give you lot. Things you lot can't touch include everything outside of this area. The near common error medical students make is to forget that their mask isn't sterile and scratch their olfactory organ! Another common pitfall is the surgical lights, which sometimes have sterile handles on them and sometimes don't – always cheque before touching them.
Before making their get-go incision, the consultant will ask the anaesthetist if they are "OK to start".
During the operation
Your function every bit an assistant
Speak clearly to other members of the team – don't whisper or mumble as nobody will be able to hear you through your mask.
Beingness an assistant is like shooting fish in a barrel. If you practice exactly what you are asked to practice and nothing else, it is very difficult to go wrong. Your main responsibilities are likely to include:
- Holding retractors – bandy hands at regular intervals to foreclose fatigue and cramps
- Cutting stitches and ties – ever ask how long they desire you to leave the ends, and whatever you do, don't cut the knot!
- "Following" suture lines to keep the tension – this is the same principle as putting your finger on a shoelace knot to keep it tight, but instead yous pull upwards in the management indicated by the surgeon
- Using suction (be gentle) and maybe the diathermy (be careful)
- Holding the camera during laparoscopic cases – try to stay as steady equally you can, and keep the surgeon'south instruments in the centre of the screen so they tin see what they're doing
If you are asked to practise something you don't hear, don't sympathise or don't know how to exercise, don't just judge. Ask the surgeon to explain exactly what they need.
No thing how confident you may experience near your knowledge of surgical instruments and procedures,never mess with the scrub nurses' tables or trays. Depending on which nurse yous are scrubbed with, this could lead to anything from a polite word in your ear to a slap on the wrist or even being told to descrub. This rule is part of full general theatre etiquette but is also of paramount importance considering the nurses need to proceed track of all the instruments for their final "count" to ensure that nothing gets left inside the patient. In most cases, if you need anything from a tray, even if it's just a mop that's easily inside your reach, information technology is good practise to enquire the scrub nurse to pass it to you rather than grabbing it yourself.
If youaccidentally touch anything non-sterile at whatever point, you volition need to modify your gloves, gown or possibly completely rescrub. Be honest if this happens, equally the patient volition be at increased risk of infection if you go desterilised and and then continue to contaminate other things with your dirty gloves, such as surgical instruments or their internal organs. Sometimes you won't even realise you've done information technology and the ever-vigilant scrub nurse volition point information technology out to you – if this happens, apologise, thank them for pointing it out and get sort yourself out without touching anything in the sterile field. Unsurprisingly, poo counts as unsterile, so try not to go it on your easily if yous can assist information technology.
If you drop something or something falls off the table onto the flooring – stray mops and forceps fall off all the fourth dimension – don't pick information technology up! Apologise and say clearly "mop on the flooring" or "forceps on the floor" so a member of the flooring team can come up and selection it up. This is very important to make sure nothing goes missing for the count.
Sharps
Doing operations on people by and large requires the occasional use of abrupt objects such as scalpel blades, needles and scissors. Sharps prophylactic is therefore absolutely paramount in theatre. Hither are some tips:
- scalpels and hollow needles are usually passed in a plastic kidney dish rather than directly hand-to-hand
- suture needles are handed over readily mounted on a needle holder and should never be touched with your hands – use a pair of forceps to selection them up and adjust their position if necessary
- when manus-tying knots, suture needles should e'er be "parked" with their point facing towards the needle holder, to stop y'all from stabbing yourself or somebody else while y'all tie
- when passing sharps dorsum to the scrub nurse, always park the needle and clearly say "needle back to yous" or "abrupt back to you" to ensure they take extra intendance
- other things you might hurt yourself on include the diathermy, which can be sharp and/or burn through gloves, orthopaedic instruments and stapling devices – one of my registrars one time got his finger stapled onto someone'due south vagina, so don't underestimate them!
If you are unfortunate enough to become a needlestick injury – which tin can all the same happen despite everyone's best efforts – say something about it immediately. Yous will demand to descrub and manage it similar whatever other needlestick by encouraging bleeding, washing information technology thoroughly and applying an antiseptic +/- a dressing. The aforementioned goes for eye-splashes. The floor nurses volition help you if you're not sure what to do. You will need to contact occupational health so they can co-ordinate take chances assessing the patient and consenting them for claret-borne virus testing – never exercise this yourself. Occupational health will also accept your blood for storage and accommodate for you to be followed upward and tested over again in 6-12 weeks. Despite it being a genuinely massive annoyance, it is very of import that you attend occupational wellness follow-up as it's your health at stake, and besides your indemnity and payment protection insurance often won't embrace you if you don't follow the process through properly.
General intraoperative survival tips
Fatigue
Long operations are very tiring, both physically and mentally, particularly if yous're not used to it. If you're on a placement where you'll be in theatre a lot, one really of import matter is to concentrate on your posture then you don't get a sore neck or back – this is both surprisingly painful and surprisingly incapacitating. Most surgeons railroad train themselves to stand with a straight back and bend simply their neck to await downwardly at the patient, as this minimises the risk of strains – try to copy how they're continuing the next time you're in theatre. Don't slouch or curve your lower back too much as this will get sore very quickly and you lot will quickly starting time to get distracted, fidgety and grumpy. Bend your knees and stand on tip-toes every so often to stop your legs from going expressionless. If you cease upwardly being asked to hold something in a ridiculously uncomfortable position, speak upward and say so, equally otherwise, you might drop things and more importantly might hurt yourself or the patient.
If and when you kickoff to ge t tired, it can be extremely tempting to take the weight off your anxiety for a little bit past leaning against part of the operating table. Please remember that there is a patient somewhere underneath all of those drapes, and they've already got enough problems without you squishing them.
If yous're completely knackered and your easily aren't currently needed for an essential part of the operation, enquire the nurses for a stool and have a trivial sit downwards at the side of the room for a few minutes. The nurses can also bring you a lovely cold drink with a straw (I personally recommend the ubiquitous NHS lemon squash) and volition even manoeuvre the straw under your mask for yous if you inquire them very nicely.
Fainting
Working in surgery is a visceral experience, in a lot of respects! Haemorrhage, whether from tiny venous oozers or massive arterial spurters, is inevitable, so don't freak outwhen this happens. Depending on the operation, you may also end upwards getting up close and personal with necrotic tissue, pus, poo or wee, which will manifestly be unpleasant and smelly at times. The easiest way to cope with this in theatre is to concentrate on breathing through your mouth and be very glad that you're wearing a mask. Information technology is worth noting that if you want to succeed in whatsoever branch of medicine, not but surgery, bleeding and bad smells are something you just have to deal with. If yous swoon at the sight of claret you probably need to consider a different career.
If you outset to feel unwell or like you might faint, DON'T ignore it and promise it will go away. In nearly cases information technology will laissez passer and you'll be fine, only information technology's not worth the risk of either a) fainting backwards onto the rock hard floor and hurting yourself, or b) even worse, fainting onto a fellow member of the squad and hurting them, or c) worst of all, fainting into an open body cavity and potentially seriously harming the patient. The nurses are well versed in how to handle nausea and lightheaded spells, and information technology may be that all you demand is a quick sit downwards for a couple of minutes and some sips of cold water. Nevertheless, they may accept yous away somewhere for a little prevarication-downwards and some toast and tea. Don't feel too embarrassed if this happens – it has happened to all of us at some point, and the team will expect much more favourably upon the banana who acts honestly and sensibly than the ane who tries to ability through and so ends upwardly faceplanting into the patient'due south intestines.
Other distractions
If you need to get to the toilet, you'll demand to weigh upwards your options and make a tactical decision. Almost of the time you'll be able to manage until the cease of the operation. However, continuing to help whilst being distracted past a massively overfilled bladder might accept implications for patient safety depending on the length and complexity of the procedure. If y'all're actually really drastic, it'southward better to descrub and relieve your discomfort, regardless of the potential eye-rolling/sighing/mockery your request might invite from the theatre squad.
Some bits of some operations are tedious. This is unfortunately unavoidable, and even surgical trainees volition sometimes get bored in the middle of a long faffy procedure. The most important affair is not to lose focus and switch off, equally you might miss important instructions or be dull to react when something unexpected occurs. Attempt thinking through the beefcake and blood supply of the area beingness operated on or the pathophysiology of the underlying disease procedure, or asking the surgeon about these. Don't outset thinking most what to take for tiffin or your upcoming epic night out on Friday, or you lot'll cease up irreversibly daydreaming and you will become defenseless out!
In that location may exist music playing in the operating theatre. If this is the case, bad karaoke is highly probable to occur and yous may be expected to participate.
Y'all will quickly acquire that there are good times and bad times to ask questions. Most consultants appreciate students beingness interested in what's going on and are more than than happy to teach. Even so, if you want to inquire something, the best time to practise it probably isn't when something big is bleeding, or when they are dissecting around something important or suturing up something very small. Don't experience bad if you lot are ignored or rebuffed every now and again – it's nothing personal, they just need to concentrate.
Counts and endmost upward
When the surgeon has finished messing near with the patient'south insides for whatever reason, they will need to close up the hole(s) that they have made. Before this can happen, the nurses need to perform their beginning count of all the instruments to ensure that everything is accounted for and nothing has been left inside the patient. This can take a little while, every bit the two people doing the count have to see every single instrument, even if it's withal in use. Effort not to disturb the nurses while they're doing this as you lot might make them lose count! When they're finished they volition tell the surgeon that the "first count is right", and the surgeon will verbally acknowledge this.
Once they know there's nothing left inside, the surgeon can safelyclose the wound. This is frequently done in several layers with severaldifferent suture materials. For instance, a midline laparotomy closure ofttimes uses a large continuous size 1 PDS for mass closure of the fascial layers, unremarkably followed by some interrupted 2/0 Vicryl to the subcutaneous fat to bring the skin edges together, then either subcuticular 3/0 Monocryl or skin clips to the skin itself. You volition exist expected to assist past retracting,cut knots and following the suture line. If you've practised suturing before and ask nicely, you might be immune to suture the peel nether supervision, which is very satisfying! If yous've never used sutures earlier, don't try to blag information technology, just say then – the surgeon may talk yous through a couple of stitches or testify you how to exercise information technology then y'all can have a go side by side time, which is much better than giving information technology a go by yourself and making an embarrassing dog's dinner of things (run across our suturing guides for more details).
When all wounds are closed and the operation is finished, the surgical field is cleaned up with wet and dry out swabs earlier dressings are applied – these are usually OpSite dressings which come in diverse sizes, often endearingly referred to as "baby", "toddler", "teenager", "adult" etc. The nurses often practice this, but when I was a educatee I used to enjoy doing it as it meant I could tell myself that I had at least contributed something useful!
At the end of the operation, the nurses perform another "concluding count" of all the instruments to make sure nothing has gone missing since the commencement 1, and inform the surgeon that the "final count is correct". They once more have to verbally acknowledge this. If an item cannot be found, the theatre is searched meticulously for it, and it ordinarily turns upwards on the floor or underneath a drape or a shoe or something. If it even so tin't exist plant, the patient needs an X-ray before they go out the theatre – this shows up pretty much all metallic instruments autonomously from microscopic suture needles, and can as well bear witness mops, packs and pledgets, which accept an 10-ray detectable stripe.
After the operation
When the operation is finished, you need to de-scrub properly. Start, remove your gown by turning it inside out and rolling it into a ball before placing it in either the dark-green laundry bin (for reusable gowns) or the orangish clinical waste bin (for dispensable gowns). Next, cheque your gloves for holes, remove them past turning them inside out to prevent claret from flicking everywhere, and place them in the orange clinical waste matter bin. Check your hands for any bloodstains or cuts that could indicate a torn glove or needlestick injury. Finally, remove your mask and identify it in the orange bin too. And then go and wash your hands thoroughly for a infinitesimal or and then – this is important for infection command and is also squeamish and refreshing if you've been stewing abroad in hot sweaty scrubs for a while.
The patient is moved dorsum onto a bed using the Patslide. Again, it is common courtesy to offering to help with this. Unless they are very unwell, they normally stay in the theatre until they have woken up enough to be extubated safely, and are then taken round to the recovery area for a period of monitoring before they go back to the ward.
The surgeons will then prepare and characterization any microbiology/histopathology samples, write the operation note and sign off the WHO checklist andconcluding count. They will need your surname to put yous on the op note as an assistant.
Ask for feedback on anything you did well or could take done ameliorate, especially if you tied some knots or did some suturing. It is useful to discuss whatsoever learning points and interesting aspects of the case to help you to understand what was done and why.
Give thanks the team for having you lot and say farewell before leaving.
If yous're on a placement for a few weeks, try and follow patients up after their operation. Go and have a chat with them on the ward to see how they're doing, and follow upwards the results of any histopathology or microbiology from samples taken in theatre. This will give you a better understanding of normal postal service-operative recovery and mutual surgical conditions.
Logbooks
Continue a logbook of operations you go to, especially if yous think you might be interested in a surgical career. Remember that your list needs to be confidential, so don't put patient names on it! You tin can either keep your own handwritten/computerised list or employ an online logbook – the best one is the Intercollegiate Surgical eLogbook by the Royal College of Surgeons which is used by all Uk surgical trainees. You need 2 unique identifiers for this, usually the patient'southward hospital/NHS number and their date of nascency. It is very satisfying to proceed a log of procedures you've seen, assisted with and performed under supervision – even little things like stitching up a wound count! You can also log more than ward-based "medical" procedures such every bit catheterisation, arterial line and key venous line insertion, pleural/ascitic taps and lumbar punctures – again, I really wish I had known this as an F1! You tin print out logbook summaries to put in your CV or portfolio, which will brand you lot seem very switched on and professional in undergraduate times of need, for example, if you are applying for a competitive summer school, elective or intercalated caste programme, or a prissy juicy bursary to comprehend elective expenses. Information technology is also relevant for task applications for a multitude of specialities, not just for surgery. For example, medics demand to perform ascitic taps and lumbar punctures, A&E docs demand to be competent at suturing and chest drains, anaesthetists need to exist able to put in lines, and GPs can independently perform a whole range of minor surgical procedures provided they have the necessary bones surgical skills.
Most teams are happy to have students forth outside of scheduled teaching lists, so if you fancy a bit more exposure don't be frightened to get in touch and ask. Most surgeons are friendly creatures who are used to students being instantly switched off past their specialty, and so they will exist overjoyed if you lot want to come and keep them company for a bit.
Summary
I hope this has been a helpful guide to the magical world of the operating theatre, and that you will find your surgical placements less intimidating and more fun as a outcome of reading it. If non, I hope that at the very least I've covered all the major mistakes that people make and then that y'all won't become in trouble – please let me know in the comments below if I've missed annihilation, or if there is anything else yous'd similar to know about.
May the forceps be with you…

Source: https://geekymedics.com/theatre-etiquette/
0 Response to "Need to Go to Plastic Surgeon to Have My Chest Incision Opened Again N Cleaned Out N Closed Up"
Post a Comment